The next in our "Best of the Month" series is from May 14, 2014:
I recently performed an autopsy on a 67-year-old man had a seven-year history of progressive difficulty with halting speech. His wife described him as seeming to be “groping for words”. Three years after initial presentation, he demonstrated profound difficulty both initiating and finishing sentences. His verbal communication was marked by jumbled grammatical errors in which he put words in the wrong order and tense. For example, when asked by his neurologist to recount his activities over the day, he responded: “Go I… the grocery store… to.” He had no difficulty with naming objects or understanding their use. He had only mild amnestic deficits and no visuospatial difficulties. During the last months of his life, he began to become more rigid in his personality and more socially withdrawn.The clinical diagnosis in this patient is primary progressive aphasia, non-fluent/agrammatic variant. The pathologic diagnosis is frontotemporal lobar degeneration with 3R tau inclusions (FTLD-tau), commonly known as Pick disease. The clinical presentation of FTLD can be divided into two types: the behavioral variant (bvFTLD) and primary progressive aphasia (PPA). Neurologists subclassify PPA into three subtypes: semantic variant (sv-PPA), non-fluent/agrammatic variant (na-PPA), and logopenic/phonologic variant (lv-PPA). While sv-PPA and na-PPA generally correspond to FTLD pathology, lv-PPA typically corresponds to Alzheimer disease (AD) pathology (and is accordingly referred to as the “language variant” of AD). The syndrome of na-PPA is characterized by predominant language dysfunction in which there is a disordering of words in sentences, an inability to repeat complex words (e.g., saying “castaphory” when asked to repeat back the word “catastrophe”), inability to construct complex sentences, and other deficits in grammar and phonology. In contrast, a diagnosis of sv-PPA is given to patients who exhibit a general deficit in their ability to understand word and object meaning. Patients with sv-PPA also show difficulty in naming objects and understanding what they are used for. A diagnosis of bvFTLD is ruled out as this patient only showed behavioral changes only late in the disease course
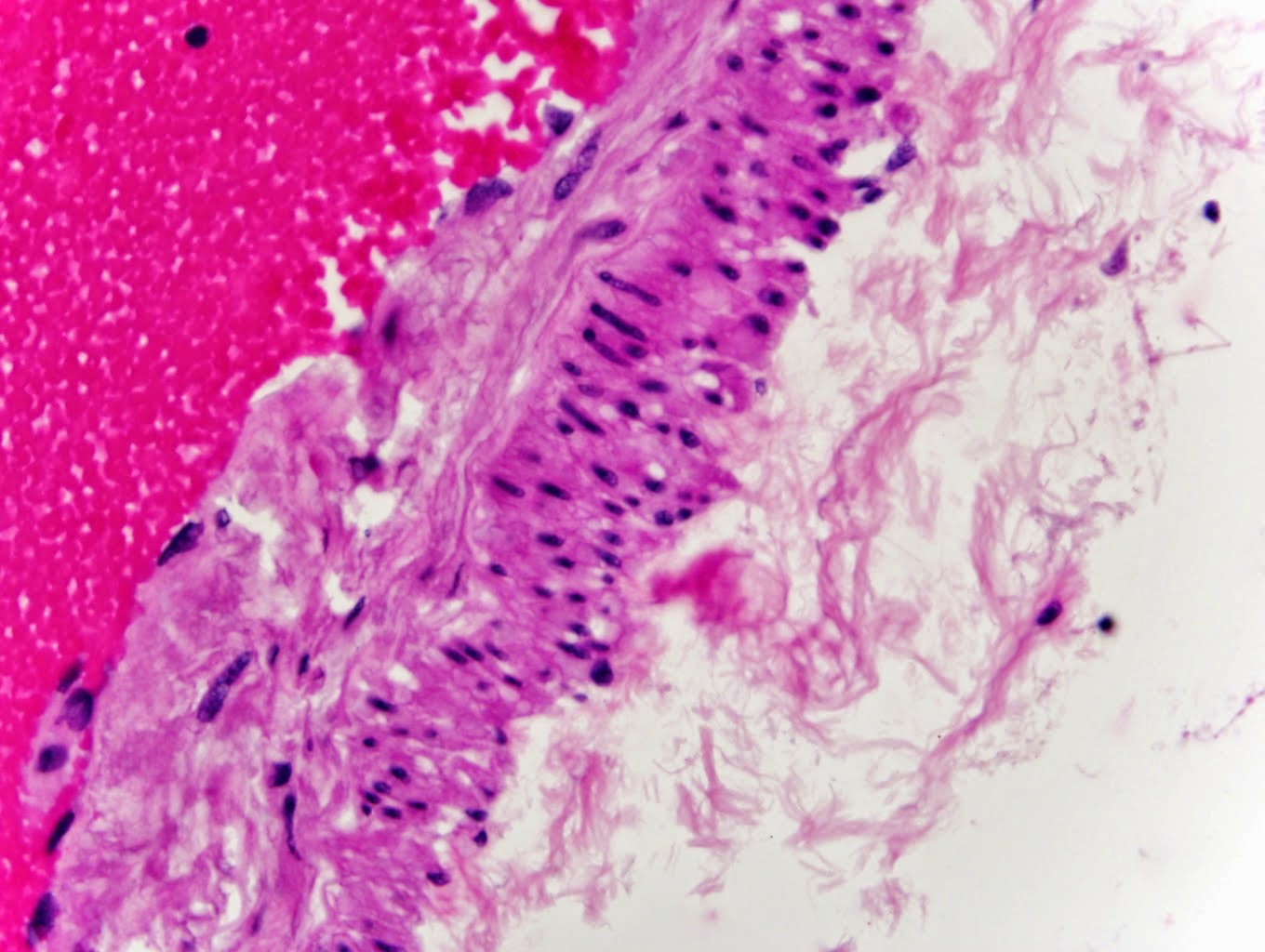
Pick disease was demonstrated pathologically by the presence of 3R tau positive Pick bodies (see photomicrograph) in the frontal and temporal lobes as well as the dentate fascia of the hippocampus, cornu Ammonis of the hippocampus, presubiculum, cingulate gyrus, insula, and inferior parietal lobe.
 |
| 3R tau positive Pick body in the inferior temporal gyrus |
For the practicing neuropathologist, FTLD’s
are not yet classified on a molecular basis (although some day they surely will be), but rather according to the particular
protein aggregation which is detected using immunohistochemistry. The five possible
FTLD subtypes, based on specific associated protein aggregations, are
represented in the following table:
FTLD
type
|
Associated
Protein Aggregation
|
FTLD-tau
|
Tau (can be further
subclassified into 3-repeat [3R], 4-repeat [4R], or 3R+4R tau)
|
FTLD-TDP
|
Transactive response DNA-binding protein of 43 kDa (TDP-43)
|
FTLD-FUS
|
Fused in sarcoma (FUS)
|
FTLD-UPS
|
Ubiquitin (with UPS standing
for ubiquitin-proteasome system)
|
FTLD-ni
|
No immunoreactivity
|
In 80% of cases of sv-PPA, the underlying histopathology is that of FTLD-TDP; while in the majority of na-PPA cases, the pathologic substrate is FTLD-tau. Although not denoting a specific clinical syndrome, the term “Pick disease” has come to denote FTLD-tau, particularly referring to aggregation of the tau isoform in which there are three repeats (3R) of the phosphate-binding domain.
References:
Sieben A, Van Langenhove T, Engelborghs S, et al. The genetics and neuropathology of frontotemporal lobar degeneration. Acta Neuropathol. 2012;124(3):353-372.